
Non-small cell lung cancer
Lung cancer - non-small cell; NSCLC
An in-depth report on the causes, diagnosis, treatment, and prevention of non-small cell lung cancer (NSCLC).
Highlights
Overview
- Lung cancer is the leading cause of cancer death in American men and women.
- Lung cancer is more deadly than colon, breast, and prostate cancers combined.
- Worldwide, lung cancer is the top cause of cancer death in men and is only surpassed by breast cancer in women.
- Non-small cell lung cancer (NSCLC) accounts for about 80% to 85% of all lung cancer cases.
Risk
- Smoking is the primary risk factor for lung cancer. Around 85% of lung cancer patients have a history of smoking.
- It is estimated that people with early stage cancer who quit smoking double their chance of survival (70%), compared to those who continue to smoke (33%).
- Examples of genetic factors that promote the growth of lung cancer cells include gene mutations in epidermal growth factor receptor (EGFR) or KRAS, as well as the ELM4-ALK gene fusion.
- Annual screening with low-dose CT scans has shown benefit in certain high risk groups of current and former smokers, and is recommended for these groups only.
Treatment
- Several surgical options, including those with tissue-sparing techniques, are available for various stages of lung cancer. Surgery is considered standard treatment for stage I and II NSCLC.
- Experts are looking at newer risk profiles with an aim toward doctor-patient decision making rather than strict treatment eligibility rules.
- Video-assisted thoracoscopic surgery (VATS) is becoming more widely used to treat early stage lung cancer patients.
- Certain tumors respond differently to specific drug therapy options. Research is now focused on protein biomarkers and gene mutations that give rise to the tumor. With this information, caregivers can match customized chemotherapy and other drug treatments for advanced NSCLC patients.
- Gefitinib (Iressa), erlotinib (Tarceva), crizotinib (Xalkori), afatinib (Gilotrif), pembrolizumab (Keytruda), osimertinib (Tagrisso), and dacomitinib (Vizimpro) are among the newer targeted biological agents being used for treatment.
- For people with advanced stage NSCLC, a palliative care program started at the time of diagnosis and continued throughout the continuum of care (combined with standard cancer treatments) has shown to improve survival, quality of life, and mood.
Introduction
Although lung cancer accounts for only 13% of all newly-diagnosed cancers in the United States, it is the leading cause of cancer death in American men and women. Globally, lung cancer is the first cause of cancer death in men and is only surpassed by breast cancer in women. It is more deadly than colon, breast, and prostate cancers combined. Over 140,000 people die from lung cancer each year. Death rates have been declining in men and women over the past decade.
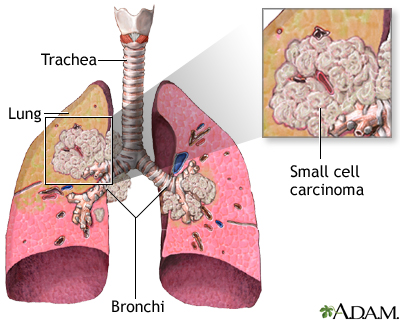
The Lungs
The lungs are 2 spongy organs surrounded by a thin moist membrane called thepleura
. Each lung is composed of smooth, shiny lobes: the right lung has 3 lobes, and the left has 2. About 90% of the lung is filled with air. Only 10% is solid tissue.- Air is carried from the
trachea
(the windpipe) into the lung through flexible airways calledbronchi
. - Like the branches of a tree, the bronchi in turn divide into over a million smaller airways called
bronchioles
. - The bronchioles lead to grape-like clusters of microscopic sacs called
alveoli
. - In each adult lung, there are about 300 million of these tiny alveoli. A thin membrane makes up the alveoli sacs. Oxygen and carbon dioxide pass through this membrane to and from
capillaries
. - Capillaries, the smallest of our blood vessels, carry blood throughout the body.
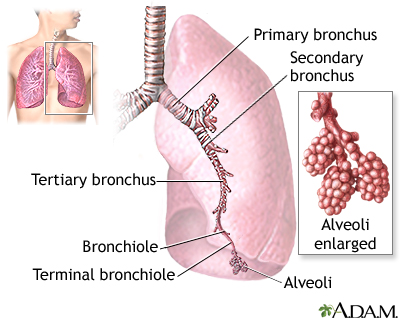
The major features of the lungs include the bronchi, the bronchioles, and the alveoli. The alveoli are the microscopic blood vessel-lined sacks in which oxygen and carbon dioxide gas are exchanged.
Lung Cancer
Lung cancer develops when genetic mutations (changes) occur in a normal cell within the lung. As a result, the cell becomes abnormal in shape and behavior, and reproduces endlessly. The abnormal cells form a tumor that, if not surgically removed, invades neighboring blood vessels and lymph nodes and spreads to nearby sites. Eventually, the cancer can spread (metastasize) to locations throughout the body.
The 2 major categories of lung cancer are small cell lung cancer (SCLC) and non-small cell lung cancer (NSCLC). Most lung cancers are non-small cell cancer, the subject of this report. Less common cancers of the lung are known as carcinoids, cylindromas, and certain sarcomas (cancer in soft tissues). Some experts believe all primary lung cancers come from a single common cancerous (malignant) stem cell. As it copies itself, that stem cell can develop into any one of these cancer types in different people. In about 40% of people with NSCLC, the cancer has spread to other areas of the body at the time of diagnosis.
In addition, cancers in the lung may have spread from other sites, such as the breast, thyroid, or colon. In these cases, doctors name the cancer after its original location, such as "breast cancer with lung metastases."
Non-Small Cell Lung Cancers (NSCLC)
NSCLCs are categorized into 3 types:
Squamous cell carcinoma
(also called epidermoid carcinoma)Adenocarcinoma
Large cell carcinoma
These separate types are grouped together because, in the early stages before the cancers have spread, they all can be treated with surgery.
Squamous Cell Carcinoma
Squamous cells are formed fromreserve cells
. These are round cells that replace injured or damaged cells in the lining (theepithelium
) of the bronchi, the major airways. Tumors formed from squamous cells are usually found in the center of the lung, either in a major lobe or in one of the main airway branches. They may grow to large sizes and form cavities in the lungs.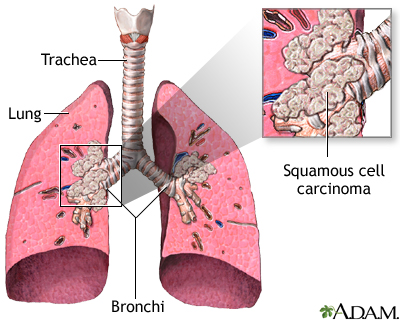
When squamous cell cancer spreads, it may travel to the bone, adrenal glands, liver, small intestine, and brain.
Squamous cell carcinoma is nearly always caused by smoking, and it used to be the most common cancer. It still makes up 25% to 30% of all lung cancers.
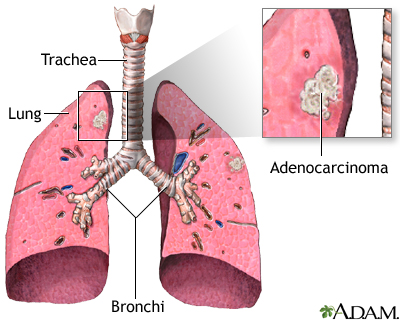
Adenocarcinoma
Adenocarcinomas usually start from the mucus-producing cells in the lung. About two thirds of adenocarcinomas develop in the outer regions of the lung, while one third develop in the center of the lung.
Adenocarcinomas are estimated to account for 40% of all lung cancers and are the most common lung cancers in many countries. They are also the most common lung cancers in women, and their rates are increasing dramatically in men. Until recently, adenocarcinoma was only weakly linked to smoking. Experts now suggest, however, that the dramatic increase in this lung cancer type in recent decades may be due to low-tar, filtered cigarettes. People who smoke these cigarettes draw tiny particles deeper into their lungs.
The course of adenocarcinomas varies widely. Most often, it develops slowly and causes few or no symptoms until it is far advanced. In some cases, however, it can be extremely aggressive and rapidly fatal. It can spread to the other lung, liver, adrenal glands, brain, and bone.
Adenocarcinoma in situ
Adenocarcinoma in situ, earlier known as bronchoalveolar lung cancer, is a subtype of adenocarcinoma. It develops as a layer of column-like cells on the lung and spreads through the airways, causing great volumes of sputum. This cancer is also increasing in incidence.
Large Cell Carcinoma
Large cell carcinoma, which makes up about 10% to 15% of lung cancers, includes cancers that cannot be identified under the microscope as squamous cell cancers or adenocarcinomas.
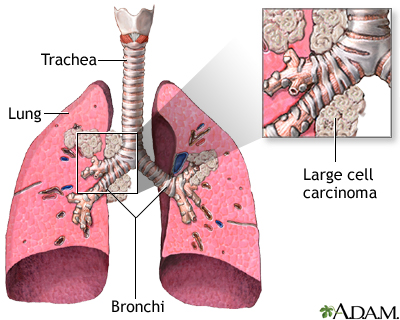
More rare types of NSCLC include pleomorphic, carcinoid tumor, salivary gland carcinoma, and unclassified carcinoma.
Small Cell Lung Cancer
Small cell lung cancer may, like squamous cells, originate from reserve cells or other cells in the epithelium. It causes 10% to 15% of all lung cancers. Without chemotherapy, it is very aggressive and usually rapidly fatal. It requires a different treatment approach from NSCLC, and it is not discussed in this report.
Causes
Cigarette Smoke
Smoking causes at least 80% of lung cancer deaths, and accounts for 30% of all cancer-related deaths. Cigarettes, nicotine, or both may contribute to lung cancer in one or more of the following ways:

- The smoke is the most dangerous component of the cigarette. Chemicals formed during smoking trigger genetic mutations that lead to cancer. When people inhale cigarette smoke, they bring into their lungs tar that includes over 4,000 chemicals, some of which are carcinogenic (cancer-causing). Other inhaled chemicals in cigarette smoke that may increase the risk for cancer include cyanide, benzene, formaldehyde, methanol, acetylene, and ammonia. Smoke also contains nitrogen oxide and carbon monoxide, both harmful gases.
- Nicotine is responsible for the addicting properties of tobacco. It is not clear if nicotine itself plays a role in the growth of cancer cells. In any case, nicotine replacement products are much, much safer than tobacco.

In general, chronic exposure to tobacco may cause an acceleration of coronary artery disease, peptic ulcer disease, reproductive disturbances, esophageal reflux, hypertension, fetal illnesses and death, and delayed wound healing.
Radon
Radon is a gas produced naturally by the breakdown of uranium. It is often present in the soil and in water and can seep into any dwelling. Radon is the second leading cause of lung cancer and accounts for roughly 10% of all cases.
Other Contributors
Toxic particles leading to precancerous changes in the lung are also found in marijuana. Multiple studies report an association between abnormal lung changes and marijuana smoking.
There is considerable debate over the lung cancer risk posed by depleted uranium used in military weapons (such as in the Gulf and Balkan conflicts).
Other lung carcinogens include asbestos, arsenic, certain petrochemicals (materials made from crude oil or natural gas), and other airborne (carried through the air) byproducts of various mining and manufacturing processes.
It is thought that occupational exposure to these carcinogens cause 9% to 15% of lung cancer cases. Outdoor air pollution is also a culprit, accounting for 1% to 2% of lung cancer cases. A combination of several of these factors can increase a person's risk to over 100%.

Genetic Mutations
Genetic mutations that cause cancer generally occur in 2 types of genes:
- Tumor-suppressor genes, which prevent cells from endlessly copying themselves.
- Proto-oncogenes, which encourage cells to keep making copies of themselves (when a proto-oncogene changes [becomes mutated], it is then called an oncogene.)
Damage to either type of gene can cause a mutation that results in uncontrolled division of cells. This uncontrolled division forms tumors.
It is unlikely that a single specific abnormality causes all lung cancer. It probably takes a variety of mutations to start the devastating chain of events leading to cancer. The following mutations are among those under investigation:
EGFR mutations.
EGFR (epidermal growth factor receptor gene) is a family of genes that can mutate and promote tumor growth. This gene mutation is often implicated in lung cancer in non-smokers. It is most common in Asian populations. HER2 is a related gene under study; it plays a role in regulating cell growth.ELM4-ALK gene fusion.
ELM4-ALK refers to the fusion of 2 different genes resulting in a protein that is found in malignant NSCLC cells that appear to promote its growth. This genetic rearrangement tends to show up in adenocarcinomas in people who have never smoked or in light smokers and younger people.BPDE-caused mutations.
The chemical BPDE, a byproduct of tobacco smoke, is involved with a number of genetic mutations, including those to an oncogene called K-ras and to 3 tumor-suppressor genes known as p53, PPP2R1B, and p16. (Tumors that contain the p53 mutation may also be more resistant to chemotherapy.)Rb mutations.
Another important contributor to lung cancer is a genetically defective protein called retinoblastoma (Rb), which is associated with very aggressive tumors. Low levels of the normal Rb gene may sometimes predict aggressive cancer, especially in people with small cell lung cancer.Abnormalities in the FHIT gene.
Such abnormalities may cause the cells lining the lung to become more vulnerable to the effects of tobacco smoke and other cancer-causing substances.Alpha1-antitrypsin mutations.
People who carry a common variation in the gene for alpha1-antitrypsin, a substance that normally protects the walls of the alveoli in the lungs, are 70% more likely to develop lung cancer than those without the mutation, regardless of their smoking history.- Many other gene mutations have been implicated including BRCA1, RAP80, RRM1, ERCC1, and TS. Scientists continue to explore the complex relationship between various genes that play a role in cell production and what environmental factors give rise to cancer.
- Specific gene mutations affecting tumor growth may provide an accurate "genetic fingerprint" that can help doctors prescribe the most effective and appropriate treatment options.
Symptoms
Lung cancer is unlikely to produce symptoms until the disease is advanced. When symptoms develop, they may result from the lung tumor itself, from its effects on tissues outside the lung, or from the spread of cancerous cells to other organs.
Initial symptoms
The first symptoms of lung cancer may include some of the following:
- Frequent bouts of pneumonia, or pneumonia that does not clear up in a normal period of time
- Coughing that does not go away or coughing up blood
- Weight loss
- Fever
- Shortness of breath
- Chest pain
- Bone pain
Symptoms of Later Stages
Later-stage symptoms and complications include the following:
Shortness of breath.
This common symptom is the result of cancer that has spread in the lung and the pleura, the membrane covering the lung.- Weakness, weight loss, and loss of appetite.
Depending on where the cancer is located or has spread to:
- Swelling in the arms and face. If tumor growth or spread of the cancer presses against the superior vena cava, which returns blood from the upper part of the body to the heart, it can cause a condition called
superior vena cava syndrome
. - Trouble swallowing. The esophagus is the pipe that takes food from the mouth to the stomach. The cancer may spread to or press against the esophagus, interfering with swallowing and nutrition.
- Hoarseness. Cancer can damage the nerves that control the voice box, causing hoarseness.
- Pain, weakness, or numbness in the arm or hand, caused by damage to the brachial plexus, a group of nerves branching from the neck. This condition is called Pancoast syndrome.
- Bronchoalveolar lung cancer may produce very large amounts of mucus.
- Some lung cancers produce substances that remove calcium from bone and release it into the bloodstream, causing a condition called
hypercalcemia
. People with this disorder can experience nausea, vomiting, constipation, weakness, confusion, and fatigue.
hyponatremia
, can produce confusion, weakness, and even seizures.
Risk Factors
Before cigarettes became popular in the beginning of the 20th century, lung cancer was rare. It now affects about 228,000 Americans per year, and some 140,000 die from it annually. The disease usually occurs in people over 50 years old. Men have a significantly greater incidence of lung cancer compared to women. On the encouraging side, the rate of lung cancer and lung cancer deaths has been declining significantly over the past decade.
Smokers and Those Exposed to Cigarette Smoke
Smoking is the primary cause of about 85% of lung cancers. The risk for lung cancer in smokers is about 20 times that of nonsmokers. The risk depends on the duration and intensity of the smoking habit, measured in combination as the number of pack years. One pack year equals the number of packs of cigarettes smoked per day, multiplied by the number of years that the person has smoked. Genetic damage in the lung occurs in nearly all chronic smokers, even if cancer has not developed.
People who smoked can be at increased risk for lung cancer more than 20 years after quitting, although the risk drops significantly even in the first year after quitting. There are benefits to quitting smoking, even for people who are well into middle age. Evidence also suggests that quitting smoking after a diagnosis of early stage lung cancer improves outcomes significantly.
Secondhand Smoke
The Environmental Protection Agency has classified secondhand smoke as a carcinogen (cancer-causing chemical). Exposure to secondhand tobacco smoke increases the risk for lung cancer in the nonsmoker by about 20% to 30%.
E cigarettes/Vaping
There is limited evidence from animal studies to support the hypothesis that long-term e-cigarette use could increase the risk of cancer. Major guidelines make little to no mention of E cigarettes as a risk factor for cancer currently.
Ethnic Differences
There may be some ethnic differences in lung cancer risk. For example, African American men have about a 20% higher risk of developing lung cancer than white men. It is not clear what factors are responsible for this higher risk. Some African Americans appear to have a genetic vulnerability to the harmful chemicals in cigarette smoke.
In China, about one third of all young male smokers will eventually die because of tobacco-related illnesses. Their risk for lung cancer, however, is much less than it is for chronic lung disease, the opposite of the Western trend. The lower rate of lung cancer among Chinese people might be due to a slow rate of clearing nicotine, which results in smoking fewer cigarettes.
Socioeconomic Differences
Low income and a lack of education have been linked to an increased risk for lung cancer. Researchers say socioeconomic status is connected to other factors involved in lung cancer risk, such as smoking, diet, and exposure to cancer-causing chemicals in the workplace.
Environmental Factors
People with High Exposure to Radon
Studies have shown that radon raises the risk of developing lung cancer in underground miners by 40%. It is unclear whether the results of these studies would apply to people exposed to radon in their homes. Homes or buildings built on landfills that contain high levels of radon are the most likely sources of this low level, chronic exposure.
A cumulative long-term exposure to radon and smoking also increases the danger. Most people move an average of 10 or 11 times over their lifetime, so the risk of developing lung cancer through radon exposure is very low in most individuals, even for those who lived for a while in areas with high radon levels. People with homes that have high radon levels and those who sleep or spend a long time in basements with detectable but moderate levels should consider taking protective measures.
Workers Highly Exposed to Carcinogens
An estimated 9,000 to 10,000 men and 900 to 1,900 women develop lung cancer each year because of occupational exposure to carcinogens. More than one half of these cases are attributable to past exposure to asbestos, which has long been known to be a risk factor formesothelioma
(cancer of the pleura, the lining around the lung) and can increase the risk for lung cancer. With better protective measures, these rates are expected to fall in the future.Other chemicals that put workers at risk for lung cancer include:
- Arsenic (insecticide and herbicide sprayers, tanners, and oil refinery workers)
- Chloromethyl methyl ether (workers exposed to certain polymers, water repellents, or products using chloride and formaldehyde)
- Chromium compounds (workers using certain alloys, paints, pigments, and preservatives)
- Depleted uranium (soldiers exposed to weapons during battlefield conditions)
- Crystalline silica
lower
lung cancer rate, despite their possible occupational exposures to risky chemicals. While this rate has traditionally been attributed to good health habits, including low tobacco use, agricultural workers' exposure to endotoxin may be responsible. Endotoxin is a component of common bacteria found in soil and animals, and it may have cancer-preventing effects on the immune system.Air Pollution
Although any risk from air pollution is very small, it nevertheless may be a contributor to those lung cancers not obviously related to smoking. Some studies have found an association between increased risk for lung cancer and long-term exposure to very small particulates, especially sulfates, in polluted air. The risk, if any, is very small.
Family History
A family history of lung cancer may play a role in increasing susceptibility to this disease. People with the family history of lung cancer have 2 to 3 times increased risk. The risk is higher in both smokers and nonsmokers. There is no association between a history of other cancers and lung cancer. Both genetic factors and secondhand smoke appear to contribute to the danger in these individuals.
Hormone Replacement Therapy
Hormone replacement therapy (HRT) does not increase lung cancer risk. However, research suggests that postmenopausal women taking combined HRT (estrogen plus progestin) may have a higher risk for death from NSCLC than women not taking hormones.
Other Diseases that Increase Risk
Smokers with emphysema or chronic inflammatory lung diseases, such as asthma, are at increased risk for lung cancer. Both smokers and nonsmokers whose lungs are scarred from recurrent lung diseases, such as pneumonia or tuberculosis, are also at increased risk, particularly for bronchoalveolar lung cancer.
Lifestyle Changes
Quitting Smoking
Quitting smoking improves lung function almost immediately. Some evidence suggests that the benefits for the lungs are even more significant for women who quit than for men. Furthermore, quitting, even after a diagnosis of lung cancer, significantly improves your chance of survival. It is estimated that people with early stage lung cancer who quit smoking have a 70% chance of survival, compared to 33% in those who continue to smoke.
It can take 20 years or longer, particularly in heavy smokers, for the risk for lung cancer to be reduced to as low as it is for nonsmokers. However, lung cancer risk starts decreasing immediately after quitting smoking, regardless of how much someone smoked. Risk continues to decrease progressively for about 30 years. Quitting is extremely difficult. There are many smoking cessation programs available that can become part of a patient's overall treatment plan. No one should be discouraged if they relapse. Everyone should keep trying to quit. With continued efforts, many people succeed.

The many methods of quitting smoking include counseling and support groups, nicotine patches, gums and sprays, and prescription medication.
At this time, perhaps the most effective method for quitting is a combination of the following:
- Nicotine replacement products that reduce withdrawal symptoms and cravings. Nicotine gum and patches are available over-the-counter, and nicotine nasal spray is available as a prescription.
- The antidepressant bupropion (Zyban, Wellbutrin), which reduces emotional effects and cravings associated with withdrawal, and improves abstinence rates.
- The drug varenicline (Chantix), which blocks nicotine receptors in the brain. This medication is very effective, but carries a risk of developing psychiatric side effects. People taking varenicline, especially those with a history of psychiatric problems, should be closely monitored for changes in mood or behavior. Chantix has been linked to a possible increase in heart problems, but since smoking is a major cause of heart disease, the benefits of using Chantix to quit appear to outweigh the possible risks.
- Professional counseling or support organizations that may, in addition to medication, help people stop smoking.
- In recent years, electronic nicotine delivery systems (e-cigarettes or e-cigs) have been advocated as another method for quitting smoking. There is not enough evidence yet with respect to the safety and efficacy of e-cigarettes for smoking cessation. Preliminary studies on dual users (cigarette and e-cigarette users) suggest that e-cigarettes might actually get in the way of quitting smoking. More studies are necessary and new regulations are expected from FDA.
During the process of quitting, and afterward, people should maintain as healthy a lifestyle as possible.
Dietary Factors
The research on diet and cancer suggests that antioxidants in certain foods may protect against the DNA damage that can lead cells to turn cancerous. It is important to note that, although studies have suggested an association between these factors and cancer risk, no cause-and-effect has been proven. It is also important to note that while the antioxidants in foods may be protective, antioxidant supplements actually increase risk in smokers. That makes a healthy diet even more desirable.
Phytochemicals
Some data suggest that diets rich in fresh fruits and vegetables may protect against lung cancer in both smokers and nonsmokers. Phytoestrogens, flavonoids, and glucosinoids are the most studied dietary elements in relationship to protection from lung cancer.

Note:
Studies on these chemicals are not consistent. It is unlikely that individual phytochemicals offer protection, but rather that any benefit comes from a collection of vitamins and plant chemicals contained in fruits and vegetables.Fats and Oils
Some studies have indicated that diets high in animal fats increase the risk for lung cancer. Others have suggested that some protection against lung cancer comes from cod liver oil, which contains omega-3 fatty acids (found in fatty fish), omega-6 fatty acids (found in flax and in soybean and canola oils), and monounsaturated oils (found in olive and canola oils). However, the ability of these substances to protect against lung cancer remains controversial, and quitting smoking remains the best advice.
Vitamin Supplements
Even in those who eat a healthful diet, smoking reduces the body's levels of a number of vitamins, importantly vitamin C. There is no evidence, however, to support any benefit from taking antioxidant supplements, including vitamins C, E, A, folate, or beta carotene.
In fact, evidence is now suggesting that high doses of vitamin C, vitamin E, and especially beta carotene supplements have harmful effects. The strongest studies on the effects of antioxidant supplements have reported anincrease
in lung cancer and overall mortality rates among smokers who took beta carotene or vitamin E supplements. This is particularly important information for smokers, who may carry precancerous or cancerous cells for years before developing the disease. The best way to get healthy levels of important nutrients is by eating healthy foods.

Trace Element Supplements
Trace elements such as zinc and selenium have been studied for potential protection against lung cancer without any clear evidence to support their benefits.

Protecting the Home against Radon
People concerned about radon in their home or area can purchase a test approved by the Environmental Protection Agency. One way to remove radon is by installing a soil suction system. It should be noted, however, that home prevention measures rarely reduce radon levels to zero. Simply sleeping by an open window reduces the risk.
Diagnostic Tests
Physical Examination
A detailed physical examination of the whole body is very important to identify or rule out the spread of cancer to other areas, and to determine the person's general condition. For example, questions about dizziness or headaches can help the doctor determine if the cancer has spread to the brain. Bone or joint pain might suggest that the cancer has spread to the bone. The doctor will also look for head and neck symptoms that might indicate other tumors. Also, the person's weight loss and ability to function are two very important factors for predicting survival following treatment. People who are mobile and have lost less than 10% of their pre-treatment weight tend to have better survival rates.
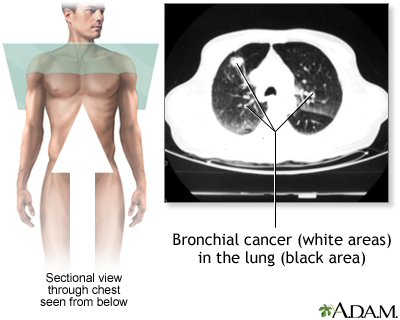
Chest X-Rays
In a small percentage of cases, a routine chest x-ray reveals the first signs of lung cancer. Usually, however, symptoms of existing lung cancer, such as coughing, chest pain, and blood in the sputum, will lead to a chest x-ray. If NSCLC is present, chest x-rays may show lesions (damaged or abnormal tissue) in the center of the lung, cavities formed by squamous cell carcinoma, or a lace-like pattern of cells spreading through the lungs. By the time lung cancer is diagnosed by chest x-rays, however, it has often spread so far that it cannot be surgically cured. Four major studies found no survival benefits in early detection from chest x-rays and sputum screening. Computed tomography (CT) scans have shown to be better than chest x-rays in detecting nodules and lung cancer. Regular screening with chest x-rays for lung cancer is therefore not recommended.
Computed Tomography (CT)
CT, particularly the specific technique called low-dose spiral (or helical) CT, is more effective than x-rays for detecting cancer in patients with suspected lung cancer. It is the standard imaging procedure for determining if and where the cancer has spread (metastasized). Surgeons also use CT scans to evaluate patients before lung surgery.
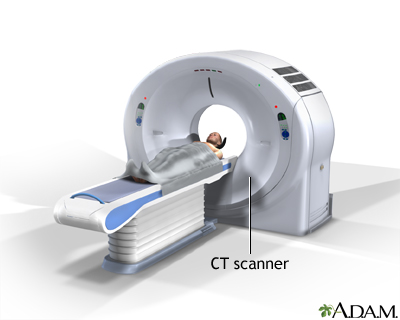
CT stands for computerized tomography. In this procedure, a thin x-ray beam is rotated around an area of the body. Using very complicated mathematical processes called algorithms, the computer generates a 3D image of a section of the body. CT scans are very detailed.
The use of helical CT for widespread early screening of people who do not show symptoms (asymptomatic) is currently under debate.
The National Lung Cancer Screening Trial found that early lung cancer detection by having low-dose CT scans yearly for 3 years led to 20% less cancer deaths in the heavy smoker group. The American Cancer Society, the American Lung Association, the National Comprehensive Cancer Network, and the U.S. Preventive Services Task Force now recommend the following:
- Annual low-dose CT screening for current and former smokers who are between the ages of 50 and 80 years, have a 20 pack-year smoking history, who still smoke or have quit within the past 15 years, and who have no history of lung cancer.
- Chest x-rays should not be offered as a screening tool.
It is important to note that screening CT scans produce many false-positive results. This means that many people have suspicious findings on a CT scan that do not turn out to be cancer after a lung biopsy is done. More research is needed to determine whether there is an overall benefit to CT screening for all smokers. People not meeting the above criteria are unlikely to benefit from lung cancer screening at this time.
Other Imaging Tests for Staging and Tracking Cancer
While CT is the standard imaging procedure for determining NSCLC, other imaging tests are also useful for staging and tracking lung cancers. Staging means finding out how advanced the cancer is.
A bone scan is done to check for spread of cancer to the bones for those with bone pain, or other findings suggesting spread of cancer to the bones.
Positron Emission Tomography (PET)
PET, specifically FDG-PET, can diagnose lung tumors as small as 1 centimeter with very high accuracy. With FDG-PET, the person is first injected with a specially formulated, radioactive liquid sugar (called FDG), and then studied with a special machine.
PET is a good imaging technique for determining the stage in patients thought to have early stage lung cancer after other testing. These people are considered candidates for surgery intended to cure. But if a PET scan identifies previously undetected spread of the cancer elsewhere in the body, the person may be able to avoid unwarranted surgery.
PET works best when used with CT scans. An imaging tool known as PET/CT is often used, which allows both types of scans to be done at the same time. However, PET/CT may also wrongly diagnose some people as having more advanced cancer than they actually have, possibly leading to the incorrect treatment.
Magnetic Resonance Imaging (MRI)
MRI, an imaging procedure that uses radio wave energy, is frequently used instead of CT scanning to locate brain and bone tumors that have spread from the lung. Importantly, since the brain always uses high amounts of sugar, a FDG-PET scan is not recommended for detecting brain metastases.
Biopsy Procedures
Biopsies of lung tissue or liquid are needed to confirm lung cancer. This requires invasive procedures that may vary from simple needle aspiration to various types of endoscopic procedures to chest surgery.
A new technique called liquid biopsy is currently being evaluated in combination with genetic testing of biopsied tissue for NSCLC diagnosis and treatment planning. This experimental approach may be especially useful for diagnosing specific mutations such as EGFR or ALK mutations in cases when the lung tumor sample is either not available or not large enough. The liquid biopsy sample used may be serum or other cell-free body fluid. Next generation sequencing (NGS) is then used to test for genetic mutations. Given that targeted agents are now available for specific mutations, detecting these mutations is important when deciding the treatment.
Needle Aspiration
Sometimes, a biopsy specimen is obtained by inserting a needle between the ribs, and then guiding it with the use of CT scans, ultrasound, or fluoroscopy (a device allowing an x-ray view). Specific techniques include transbronchial or transthoracic needle aspiration (TBNA or TTNA), endoscopic ultrasound-guided needle aspiration (EUS-NA) and transesophageal endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA). Their use depends on how much of the area can be observed with less invasive imaging methods. There is a 5% to 10% risk for bleeding or collapsed lung with needle aspiration.
Thoracoscopy
Thoracoscopy is usually very effective for diagnosing cancer in the outer areas of the lungs, or those involving the pleura (membrane surrounding the lungs). This is a surgical procedure that uses a fiber optic tube to view the area. The procedure requires general anesthesia. The surgeon passes surgical instruments and a fiber optic tube through a small incision in the chest. The tube has a camera in it, which allows the surgeon to look at the lungs on a video screen.
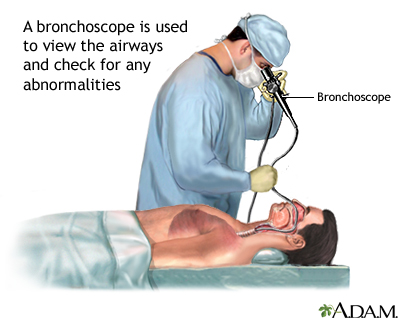
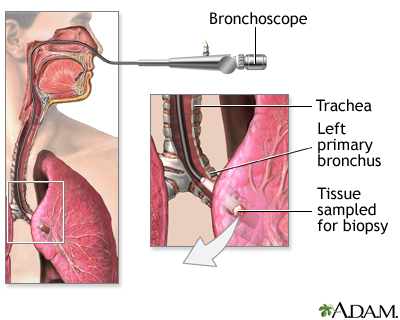
Bronchoscopy
Bronchoscopy can help locate cancer that develops in the central areas and major airways of the lung (usually squamous or small-cell cancer). The procedure is done as follows:
- The person is given a local anesthetic, oxygen, and sedatives.
- The doctor inserts a bronchoscope, a hollow flexible tube, often containing a fiber optic light source, into the lower respiratory tract through the nose or mouth.
- The tube acts like a telescope into the body, allowing the doctor to see the windpipe and major airways. In a procedure called fluorescence bronchoscopy, the doctor injects the person with a drug that makes cancer tissue appear red when exposed to laser light from the bronchoscope.
- The surgeon removes specimens for biopsy, ideally combining techniques to include cutting tissue, brushings, and a washing process called bronchoalveolar lavage (BAL). BAL involves injecting saline through the bronchoscope into the lung and then immediately suctioning the fluid back through the hollow tube of the bronchoscope. The fluid is then analyzed in the laboratory. Both brushing and washing procedures may be very valuable additions to this procedure.
Bronchoscopy is usually very safe, but complications can occur. They include:
- Allergic reactions to the sedatives or anesthetics
- Asthma attacks in susceptible patients
- Bleeding
People may develop a fever after the procedure.
Mediastinoscopy
Mediastinoscopy uses a tube inserted in the central part of the chest to locate the appropriate areas for biopsy. It is performed if the physician suspects that cancer has spread to nearby lymph nodes but has not yet spread to other parts of the body, and to confirm negative biopsy results. This procedure is slowly being replaced by endoscopic ultrasound and endobronchial ultrasound methods, as well as video mediastinoscopy.
Endoscopic Ultrasound (EUS) and Endobronchial Ultrasound (EBUS)
In EUS and EBUS, an ultrasound guided endoscope or bronchoscope is passed through the mouth into the trachea. No incisions are needed. The airway and surrounding structures and lymph nodes can be viewed and sampled with these techniques. The tests are highly accurate and often complement FDG-PET in staging. Performed together, the tests are more sensitive than either alone, and may become the next gold standard in lung cancer staging.
Laboratory Tests
Sputum Analysis for Presence of Cancer Cells (Sputum Cytology)
Analysis of coughed-up sputum, performed as a screening test for lung cancer, is often done along with chest x-rays. This method has not reduced death rates. Recent improvements in this screening technique are under study.
Sputum analysis may also be used to diagnose lung cancer in someone with signs of lung cancer. However, it is not 100% accurate. If a sputum analysis does not show cancer cells, other tests are performed.
Biomarkers
Biologic markers, called biomarkers, are high levels of substances that are released by tumors and indicate the presence of specific cancers. Biomarkers can be found in sputum, blood, and tissue samples. They can include:
- Proteins
- Enzymes
- Hormones
- Amino-acid compounds
- Antigens (identified by antibodies that specifically target them)
- Growth factors
- Other chemicals
A number of these biomarkers are being evaluated alone or in combination as either screening tools or as potential markers for the risk of disease progression. Some of these biomarkers may be detectable 1 to 3 years before a clinical diagnosis of lung cancer. The potential for this early diagnosis could mean an improvement in lung cancer survival in the future.
Other Tests
As part of the doctor's initial examination, patients may have a pulmonary function test and breath analysis to evaluate lung health and capacity. The doctor may also take a complete history of the heart and lungs, because they are often involved in complications following lung cancer surgery.
Staging Systems
In lung cancer, the stage of the disease at the time of diagnosis is a major factor in determining how to treat the cancer, and how long the person can expect to live. In general, survival is longest for people with very early-stage disease and shortest for people with very advanced disease that has spread to several areas of the body. However, some groupings with very different clinical features can have similar prognosis. Staging is based on the results of physical and surgical examinations, and laboratory and imaging tests, including biopsies. A combined approach is necessary for accurate staging. Research has shown that endosonography plus surgical staging produced more accurate staging results than surgical staging alone.
To determine the stage, medical professionals first categorize each tumor by size and by how far it has extended. This identification method is called the TNM system.
The TNM categories then determine the stage (numbered 0 to IV) of the cancer.
The TNM System
TNM stands for:
- TUMOR
- Regional lymph NODES
- METASTASIS (cancer spread beyond the original tumor)
T refers to the size and spread of the tumor
In TX and T0 staging, the tumor either cannot be assessed or is indicated by cancer cells in sputum or lung samples, but it cannot be seen.
In Tis, or carcinoma in situ, the cells are cancerous, but the tumor does not show evidence of spreading.
You may see T1, T2, T3, or T4. The higher number indicates that the tumor is larger and may involve more areas of the lung or chest:
- The main airway
- Chest wall
- Diaphragm
Other signs of more advanced tumors are:
- The tumor is associated with a collapsed lung or swelling that blocks the entire lung.
- The tumor is accompanied by an increased amount of fluid between the pleural membrane and the lung.
N refers to the degree of cancer spread to the regional (in the area of tumor) lymph nodes
- In stage NX, the regional lymph nodes cannot be assessed.
- In stage N0, the regional lymph nodes are still cancer-free.
- In N1, N2, or N3 the cancer has spread to lymph nodes, anywhere from those that are nearest to the tumor, those near the lung where the tumor is located, or those farther away in the chest or near the other lung or up by the collar.
M Stages refer to cancer spread (metastasis)
- In M0, spread has not occurred.
- In M1a, tumor nodules are present in the other lung or on the pleura (the sac surrounding the lungs), or a malignant pleural effusion (cancer cells in the fluid within the pleura) is present.
- In M1b, distant spread has occurred.
Other Factors Determining Treatment Choices and Outcome
Staging factors are used to help determine treatment and outlook. The following suggest a more aggressive disease:
- The presence of respiratory symptoms
- A tumor larger than 3 cm
- High numbers of blood vessels in the tumor
Researchers are always looking for more accurate ways to determine lung cancer treatment and outlook, such as specific biomarkers and related blood vessel development within tumors. These markers might eventually help predict the cancer's aggressiveness and determine the best treatment approach.
Using the TNM information, lung cancer is divided into stages, I through IV. Stages I through III are further divided into A or B (for example stage IA and IB). Each stage will usually have a different approach to treatment.
Treatment Options by Stages
Occult Stage
In the occult stage (TX, N0, M0), cancer cells are found in a sample of a person's coughed-up sputum, but no cancer cells have yet been detected in the lung.
Treatment Options
Surgically removing the tumor (if one can be located) can allow doctors to identify the stage, and often results in a cure. Video-assisted thoracoscopy is a less traumatic procedure compared to open surgery. People who are too frail for surgery may consider stereotactic body radiotherapy as an alternative.
Stage 0 or Carcinoma in Situ
Stage 0 or carcinoma in situ (Tis, N0, M0) are noninvasive cancers. Only a few layers of cancer cells are detected within one local area. The cancer has not grown through to the top lining in the lung and can be surgically removed. However, there is high risk for development of a second tumor.
Treatment Options:
- Surgery (discussed in more detail below), often a limited procedure, where only part of a lobe is removed from the lung.
- In people who cannot be treated surgically, photodynamic therapy, cryotherapy, or brachytherapy (discussed below) are possible treatments.
Stage I
In stage I, the cancer has reached the higher layers of the lung but has not spread into the lymph nodes or beyond the lung. Stage I is divided into stage IA and stage IB.
General Treatment Options
The primary treatment is surgery, such as lobectomy (removal of a whole lobe), if possible. People with poor lung function should have partial lobectomy, if possible. Radiation treatments may be appropriate and beneficial for people who cannot have surgery. It is not clear if early-stage lung cancer patients who have radiation or chemotherapy in addition to surgery have higher survival rates.
Treatment for stage IA and stage IB lung cancer includes:
- Lobectomy or sometimes pneumonectomy (removal of one lung.)
- Wedge or segment removal, particularly in patients with poor lung function who cannot handle lobectomy.
- Radiation in selected people who cannot have surgery or whose cancer cannot be fully removed.
In general, chemotherapy is not done following surgery unless the tumor is not completely removed.
The overall 5-year survival rates for early stage-cancer are around 60% to 70%. People should consider smoking cessation programs and clinical trials to prevent cancer from returning after the initial treatment. The risk for recurrence is highest in patients who continue to smoke.
Stage II
In stage II, the cancer cells have spread to nearby lymph nodes.
General Treatment Options
Surgery, usually a removal of the involved lobe (lobectomy) or the entire lung (pneumonectomy), is the treatment of choice. Radiation treatment after surgery does not seem to improve survival, but may be performed after an incomplete surgical procedure.
If the tumor is completely removed, radiation therapy is usually not performed after surgery. People whose cancer is inoperable may consider radiation and chemotherapy treatments.
People who do well after surgical removal of the tumor often receive a platinum-based chemotherapy regimen. Sometimes chemotherapy is considered before surgery as well.
In people who can complete treatment, 5-year survival rates average around 35% to 45%.
Stage III
In stage III, the cancer cells have spread beyond the lung to the chest wall, diaphragm, or further lymph nodes, such as those in the neck.
Generally, the treatment options for stage III tumors are:
- Surgery, if the tumor and affected lymph nodes can be completely removed. The value of surgery in these people is often debated. The fact that techniques are improving at the same time adds to the complexity of the debate.
- Targeted therapy such as pembrolizumab (Keytruda) may be considered for stage III patients who are not candidates for surgery, chemotherapy, or radiation.
- Consider chemotherapy or radiation therapy before or after surgery, or both.
- Consider clinical trials using advanced radiation techniques, including continuous hyperfractionated accelerated radiation, or 3D conformal radiation (discussed below.)
- Consider other clinical trials, including those of various combination treatments, preventive radiation therapy to the brain and new drugs.
Combination approaches may be significantly more effective than single treatments.
Stage IIIA
Researchers have confirmed good survival rates with surgery after chemotherapy and radiation therapy. However, surgery may not be an acceptable option for other patients with stage IIIB cancer in which case chemotherapy is typically combined with radiation, followed by immunotherapy with durvalumab.
Stage IIIB
Some people may consider surgery if the lymph nodes are not involved (T4, N0), and the tumor can be removed. Surgery may not be an acceptable option for other patients with stage IIIB cancer in which case chemotherapy is typically combined with radiation, followed by immunotherapy with durvalumab.
Stage IV
In stage IV (any T, any N, M1), the cancer has spread (metastasized) to other parts of the body.
Combination of 2- or 3-drug regimes that include platinum-based drugs and newer biologic immunotherapy drugs may be used:
- The best candidates are people in otherwise good health.
- Chemotherapy is not recommended for people who are too ill.
- Common chemotherapy drugs used include: platinum (cisplatin or carboplatin) and paclitaxel (Taxol, Onxal), gemcitabine (Gemzar), docetaxel (Docefrez), vinorelbine (Navelbine), protein-bound paclitaxel (Abraxane), and pemetrexed (Alimta).
- The most common immunotherapy drug is pembrolizumab (Keytruda).
- Response to any drug used is monitored.
- Some people are candidates for ongoing maintenance chemotherapy after the initial more intensive treatments.
Examples of newer targeted drugs that have been developed for treating lung cancer include:
- Bevacizumab (Avastin) may be used for patients with unresectable non-squamous NSCLC, in combination with chemotherapy.
- Ramucirumab (Cyramza) may be given in combination with chemotherapy after other types of therapy stop working.
- Customized treatments based on genetic or protein markers on the tumor include drugs such as: gefitinib (Iressa), erlotinib (Tarceva), afatinib (Gilotrif), or dacomitinimb (Vizimpro) for people with EGFR mutations and crizotinib (Xalkori) for EML4-ALK translocated NSCLC.
- People can also check government websites for clinical trials of newer drugs.
Non-drug treatments include:
- Endobronchial laser therapy
- Brachytherapy (placement of radiation source inside or close to the tumor)
- External-beam radiation for symptom relief
Treatment of brain metastases depend on size, location, and number:
- If metastasized cancer involves a limited number of sites in the brain under 4 cm, it may respond to stereotactic radiosurgery (an outpatient procedure without anesthesia using highly targeted radiation to specific areas.)
- Larger tumors are candidates for resection with radiation therapy.
Recurring or Additional New Tumors
Recurring or new tumors occur (usually in the lung again) in half of treated patients. Research shows that a single tumor in the lung is more often a new tumor that, in many cases, may be operable.
Treatment Options include:
- Radiation for symptom control.
- Chemotherapy or biologic/targeted agents.
- Laser therapy or interstitial radiation for tumors inside the airways.
- Stereotactic radiosurgery (in a few selected people) or standard brain radiation.
Surgical Procedures
Surgery is considered in the following circumstances:
- The surgical removal of an entire lobe or parts of a lung is the primary treatment for eligible people in the early stages of cancer. Recurrence is high after surgery.
- Some people with stage IIIA cancer may also benefit from surgery.
- Surgery is not out of the question in rare cases of metastasis when the cancer appears in a single operable location, such as the brain.
Surgery is often combined with other treatment options. Unfortunately, lung surgery may be too risky for patients with other lung diseases or serious medical conditions, and because lung cancers tend to occur in smokers over 50, such health problems are likely to be present. Long-term survival rates appear to be better in people treated at hospitals that perform large numbers of lung cancer surgeries, and when surgeries are performed by thoracic surgeons.
Newer risk profiles for surgery are being looked at, and people are participating in decisions about surgery based on the likely risks and benefits.
Standard Surgical Procedures
The type of surgery a person needs depends on the amount of lung or other tissue that needs to be removed.
Lobectomy
Removal of one of the lobes of the lung is called lobectomy. The person must have satisfactory lung function to undergo this procedure. The person has a 3% to 5% risk of death after this operation, with older people having the highest risk.
Wedge Resection or Segmentectomy
Wedge resection and segmentectomy remove only a small part of the lung. They preserve almost normal breathing function after the operation.

Pneumonectomy
Pneumonectomy removes the entire lung. The person has a 5% to 8% risk for death after this procedure. Older people have the greatest risk, and they almost always have a recurrence.
These surgeries may be combined with other surgical techniques such as lymphadenectomy and bronchoplasty to repair or remove additional diseased tissue.
Other Procedures
Surgical advances are allowing a wider range of options, including minimal surgeries for early cancers and surgeries that relieve cancer symptoms in the late stages of the disease.
Thoracoscopy
Thoracoscopy, also known asvideo-assisted thoracic surgery (VATS)
, is a less-invasive technique that uses a thin tube containing a miniature camera and surgical instruments. It involves much smaller incisions than open surgery (thoracotomy) and speeds recovery to the point that people are up within hours. Though the procedure is not appropriate in all cases, it offers significant advantages, especially in older or frail people. The death and complication rates following VATS are lower than those after conventional surgeries. Pain is less, and people are released from the hospital quicker. The number of VATS surgeries has steadily increased every year as physicians gain experience with the technique. Initially it was primarily used in wedge resections, but is now used for lobectomies and segmentectomies as well.Laser Surgery
Laser surgery removes small amounts of lung tissue, and it is useful for improving symptoms in stage II and IIIA patients. Laser surgery may also be beneficial in treating cancers that have spread to, and are obstructing, the throat.
Photodynamic Therapy
Photodynamic therapy uses bronchoscopy and special laser light beams combined with a light-sensitive drug, called porfimer sodium (Photofrin), to kill cancer cells. The most common side effect is sun sensitivity. Bleeding in the lungs is a more serious side effect. Photodynamic therapy may be considered for people in early-stage disease who are not candidates for other surgical procedures. It may also be used to reduce symptoms in late-stage disease.
Cryosurgery
Cryosurgery uses a probe chilled to below freezing to destroy the tumor cells on contact. It is being investigated in combination with radiation therapy. It may also be an alternative in early stage cancer for patients who cannot have surgery.
Electric Cauterization and Thermal Ablation
Electric cauterization, which uses electricity to produce heat that destroys tissue, is also under investigation as a treatment for early-stage disease.
Radiofrequency Ablation
This non-surgical technique that uses an x-ray guided electrode to deliver heat to tissues may benefit lung cancer patients who do not accept surgery, or are not eligible for surgery, radiation, or chemotherapy. Because the technique spares damage to nearby tissues, people tend to have minimal side effects. More research is needed to confirm the benefit of radiofrequency ablation over other, nonsurgical treatment options.
Radiation Treatments
In addition to surgery, radiation is the other primary treatment for early-stage lung cancer. Doctors are also studying the benefits of radiation treatment in advanced lung cancer.
Radical Radiation in Early-Stage Cancer
Radical radiation is used as the sole procedure in stage I and some stage II patients who, for medical reasons, cannot be treated with surgery. Chest radiation therapy such as conventional radiotherapy or stereotactic body radiation (highly targeted radiation to specific areas) therapy may be performed.
Combined Treatments for Improving Survival in Advanced Cancer
Radiation is also being investigated in various combinations with chemotherapy, surgery, or both. Radiation treatment plus platinum-based chemotherapy may extend survival times in advanced lung cancer. Other combinations are also showing promise.
Palliative Radiation
Doctors use palliative radiation to shrink tumors and reduce pain and symptoms. Palliative radiation is appropriate for people with advanced disease and poor lung function, or for those with cancer that has spread. In up to 85% of people with advanced disease, palliative radiation therapy helps relieve pain, shortness of breath, superior vena cava syndrome, coughing up blood, and symptoms caused by cancer that has spread to the brain.
Delaying radiation therapy until symptoms develop in patients with minimal or no symptoms does not appear to reduce survival times or impair quality of life compared to starting it right away.
Radiation Therapy in Metastasis to the Brain
Radiation is the primary treatment when cancer has spread to the brain, unless the cancer is limited enough to be treated surgically. When radiation is used, a technique called stereotactic radiosurgery may deliver powerful, highly targeted radiation to specific areas in the brain. The procedure takes about 30 minutes to 1 hour and people typically go home the same day. Up to 5 sessions may be performed.
Some trials are investigating the benefits of radiation to the head toprevent
the cancer from damaging the brain.Standard Radiation Procedures
The goal of radiation treatment is to administer doses as high as possible to kill as many cancer cells as possible, without destroying surrounding healthy tissues or causing a dangerous reaction. Doctors may try different procedures for the same patient. The exact radiation procedure depends on the site of the cancer or how far it has spread.
External-Beam Radiation.
External-beam radiation therapy focuses a beam of radiation directly on the tumor. It is generally used for cancer that has spread.Brachytherapy.
Brachytherapy implants radioactive seeds through thin tubes directly into the cancer sites. Brachytherapy may be used for lung cancers that have spread to the throat and caused obstruction. High-dose-rate brachytherapy may also have some value for people with inoperable tumors in the central region of the lung.
Hyperfractionated Radiotherapy
Hyperfractionated radiotherapy gives smaller-than-standard doses a number of times a day (usually 2 or 3). This allows doctors to use a higher dose over the whole course of treatment. It is not as useful as therapy by itself, but can have survival benefits when combined with chemotherapy.
Continuous Hyperfractionated Accelerated Radiotherapy (CHART)
CHART administers multiple doses of radiation per day but uses the standard doses. This allows the total dose of radiation to be administered over a shorter time period than the standard 6 weeks. CHART may give people with localized cancer better survival rates than standard radiotherapy or non-accelerated hyperfractionated radiation. It can cause severe swallowing problems, though. Modifying the treatment by stopping it for 2 days out of 7 may help reduce this effect.
Three-Dimensional Conformal Radiotherapy
Three-dimensional (3D) conformal radiotherapy delivers external-beam radiation specifically to targeted organs or tissues. This allows doctors to administer significantly higher doses to attack the cancer, while reducing the risk to healthy cells. This technique is generally considered the standard method of delivering radiation to lung tumors.
Side Effects of Radiation Therapy
Radiation can have significant side effects when used as part of intensive treatments, such as hyperfractionated radiotherapy or radiotherapy in combination with chemotherapy. Among the most serious problems is severe inflammation in the esophagus (esophagitis) or lungs (pneumonitis). Infection is also a danger.
The use of targeted approaches, such as conformal radiotherapy, may help reduce these complications.
Chemotherapy Treatments
Chemotherapy is the use of drugs given by injection to destroy cancer cells that may have spread beyond the tumor. Earlier, there were some doubts about the effectiveness of chemotherapy for lung cancer. However, a major analysis of 52 trials supported its use, particularly with platinum-based regimens, and with the combination of supportive care and sometimes surgery. Chemotherapy can offer an improvement in survival for several stages of lung cancer.
- Chemotherapy in early stages. Chemotherapy is proving to be beneficial in many people as an additional (adjuvant) treatment with surgery or radiation. Postoperative chemotherapy appears to provide significant benefits in overall survival, time and risk for recurrence, mainly with stage IB-IIIA.
- Chemotherapy in advanced disease. Chemotherapy may be used as first-line treatment in people with inoperable or metastasized lung cancer. It is typically used in late stages to reduce symptoms and extend survival.
Chemotherapy Drugs
Most chemotherapy regimens use platinum compounds, either cisplatin (Platinol) or carboplatin (Paraplatin). The preferred regimen uses 2 drugs, one of which is a platinum-based drug. Combinations may include drugs such as paclitaxel (Taxol) and carboplatin (Paraplatin) or cisplatin (Platinol). This regimen can also include gemcitabine (Gemzar), docetaxel (Docefrez, Taxotere), vinorelbine (Navelbine), or pemetrexed (Alimta).
Pemetrexed (Alimta), known as an anti-folate, is a chemotherapy drug for first-line treatment of advanced nonsquamous NSCLC, in combination with cisplatin (Platinol) or carboplatin (Paraplatin). The drug targets a number of enzymes that play a role in how cancer cells increase in numbers. Pemetrexed does have some serious toxic effects, but they can be significantly reduced with folic acid and vitamin B12 supplements.
Targeted Agents
Targeted agents are drugs that work by inhibiting a specific gene or protein that contributes to cancer growth or spreading. Examples of targets include receptor tyrosine kinases like the epidermal growth factor receptor (EGFR) and the anaplastic lymphoma kinase (ALK), or angiogenesis factors like the vascular endothelial growth factor (VEGF.)
Tyrosine kinase proteins control the growth of cancer cells. Gefitinib (Iressa) and erlotinib (Tarceva) are examples of this type of medication.
- Gefitinib (Iressa), afatinib (Gilotrif), erlotinib (Tarceva), dacomitinib (Vizimpro), and osimertinib (Tagrisso) are approved as first-line treatment in patients with metastatic NSCLC and EGFR mutations.
Crizotinib (Xalkori) is approved to treat NSCLC that is locally advanced or has spread to other parts of the body. It is used in people who have a chromosome change that involves the ELM4-ALK gene fusion. Resistance to the drug is common after months to years of treatment.
Ceritinib (Zykadia) is another ALK inhibitor which was approved by the FDA for the treatment of ALK-positive metastatic non-small cell lung cancer (NSCLC) in patients who failed treatment with crizotinib.
Other FDA-approved drugs that target cancer cells with ALK gene changes include alectinib (Alecensa), brigatinib (Alunbrig), and lorlatinib (Lorbrena.)
Another agent, bevacizumab (Avastin) is combined with platinum-based chemotherapy as a first-line treatment choice for people with advanced, non-squamous cancer. Bevacizumab (Avastin) is a monoclonal antibody (MAb) which inhibits growth of new blood vessels by blocking the vascular endothelial growth factor (VEGF.)
Ramucirumab (Cyramza) works by inhibiting tumor blood vessel formation in a similar way, by blocking the receptor for VEGF. It was approved to use together with chemotherapy for the treatment of recurrent locally advanced or metastatic NSCLC.
Pembrolizumab (Keytruda) was originally approved for patients with locally advanced or metastatic NSCLC who have had at least one chemotherapy regimen and whose tumors express PD-L1. In 2019, the FDA expanded this drug approval to first-line treatment for patients with stage III NSCLC who cannot be treated surgically and for patients with metastatic NSCLC. This drug blocks programmed-death protein 1 (PD-1), which may induce an immune response in the body against the tumor. Pembrolizumab may also be used alone as first-line therapy in patients whose tumors express a high level of PD-L1 or as first-line together with chemotherapy in patients without high level PD-L1 expression.
Nivolumab (Opdivo) is another antibody that blocks PD-1. It is approved for treatment of patients with metastatic squamous or non-squamous NSCLC after progression on platinum-based chemotherapy.
A combination of dabrafenib (Tafinlar) and trametinib (Mekinist) is approved for advanced NSCLC that has spread to the other parts of the body. This combination is to only be used in people with NSCLC who also have BRAF V600E mutation, a gene mutation that is associated with lung cancer.
Researchers are looking at genetic mutations and the effectiveness of several customized chemotherapy options for specific mutations.
Administration, Timing, and Drug Sequences
Chemotherapy treatments are usually performed in an outpatient setting. They are given in regular cycles for several months.
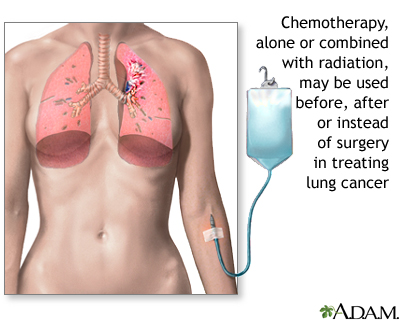
Treatment for lung cancer depends on the type of cancer and the stage of the disease. Chemotherapy is a form of treatment for lung cancer that may cure, shrink, or keep the cancer from spreading.
Side Effects
Side effects of chemotherapy treatments are common, and they are more severe with higher doses. Some side effects increase over the course of treatment.
Common side effects include the following:
- Diarrhea.
- Temporary hair loss.
- Weight loss.
- Fatigue.
- Depression.
- Nausea and vomiting. Drugs known as serotonin antagonists can relieve these 2 side effects. Serotonin antagonists work well in nearly all patients given moderate chemotherapy drugs, and in most people who take more powerful drugs.
- Anemia. An abnormally low number of red blood cells are common in lung cancer. One treatment involves transfusions or injections of erythropoietin, a drug that increases red blood cell production. Erythropoietin is available as epoetin alfa (Epogen, Procrit) and darbepoetin alfa (Aranesp), which requires fewer injections. These drugs are recommended when a person's hemoglobin level falls below a certain level, usually less than 10 g/dL.
These side effects are nearly always temporary. Most people are able to continue with their normal activities for all but perhaps 1 or 2 days per month.
Serious complications of chemotherapy can also occur, and vary depending on the specific drugs. These complications include:
- Increased chance for infection from suppression of the immune system.
- Severe drop in white blood cells (neutropenia). Certain chemotherapy drugs, such as taxanes, pose a higher risk for this complication than other drugs. A granulocyte colony-stimulating factor called filgrastim (Neupogen) can improve the white blood cell count.
- Liver and kidney damage.
- Abnormal blood clotting (thrombocytopenia).
- Allergic reaction.
Second-Line Chemotherapy
Second-line chemotherapy is used for people whose cancers have come back after the first round of chemotherapy. Several of these agents listed below have prolonged survival for people with NSCLC. Unfortunately, this survival benefit is usually only a matter of several months. Efforts are under way to identify which patients are more likely to benefit from these therapies. Because platinum-based agents are most often used first, they are not beneficial for second-line therapy.
Commonly used second-line agents include:
Docetaxel (Taxotere).
Docetaxel is usually given every 21 days. This regimen causes more side effects than pemetrexed (Alimta). Weekly doses of docetaxel (Taxotere) are effective and less toxic than the 3-week schedule.Pemetrexed (Alimta).
Pemetrexed, a first-line treatment of nonsquamous NSCLC in combination with cisplatin (Platinol), is also approved as a single second-line treatment of the same type of cancer. It is less toxic than docetaxel (Taxotere).
Combinations of Chemotherapy with Surgery, Radiation Therapy, or Both
Different combinations of treatments are considered, particularly for more aggressive or advanced cancers, different combinations of surgery, chemotherapy, and radiation therapy may be tried. These include:
- Chemotherapy following surgery (adjuvant chemotherapy). Evidence is now supporting the use of platinum-based chemotherapy after surgery in some people with lung cancers. Not all studies confirm survival benefits, however, trials are ongoing.
- Chemotherapy before surgery (induction or neoadjuvant chemotherapy). Induction chemotherapy may be used to shrink tumors before surgery. Studies have been mixed as to whether there are any survival benefits in patients with advanced lung cancer.
- Combined and multi-modal Therapy. In more advanced cancers, investigators are researching very intensive treatments that use 2 or more combinations of chemotherapy, radiation, and surgery. For example, radiation plus chemotherapy may be helpful in people whose tumors are surgically removable. Such approaches are very toxic but appear to improve survival in selected people.
Severe inflammation in the esophagus is the most common severe side effect of the radiation and chemotherapy combination. There is also a very high risk of developing serious infections, including pneumonia.
Although people over 70 may suffer more from toxic effects than younger people, studies now suggest that they can achieve survival rates with combined treatments that are equal to those in younger people.
Agents Used for Pain Relief
There are many painkilling medications available. Research shows that aggressive pain relief can help patients better manage cancer treatment symptoms. For example, reducing pain in older people with cancer may markedly lower their fatigue levels, and improve other symptoms as well.
Opioids are the most potent painkillers. The correct dosing, timing, and use of these strong medications is very important for reaching acceptable pain relief and preventing a toxic response. Patients on opioid medications should be closely monitored to prevent abuse and addiction.
Resources
- National Cancer Institute -- www.cancer.gov
- American Cancer Society -- www.cancer.org
- Cancer Care -- www.cancercare.org
- American Lung Association -- www.lung.org
- American Society of Clinical Oncology -- www.asco.org
- G02 Foundation for Lung Cancer -- go2foundation.org
- Lungcancer.org -- www.lungcancer.org
- National Comprehensive Cancer Network -- www.nccn.org
- EPA - Radon -- www.epa.gov/radon
- ClinicalTrials.gov -- www.clinicaltrials.gov
- National Cancer Institute Clinical Trials -- www.cancer.gov/about-cancer/treatment/clinical-trials
References
Alberg AJ, Brock MV, Ford JG, Samet JM, Spivack SD. Epidemiology of lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 Suppl):e1S-e29S. PMID: 23649439 www.ncbi.nlm.nih.gov/pubmed/23649439.
Araujo LH, Horn L, Merritt RE, Shilo K, Xu-Welliver M, Carbone DP. Cancer of the lung: non-small cell lung cancer and small cell lung cancer. In: Niederhuber JE, Armitage JO, Kastan MB, Doroshow JH, Tepper JE, eds. Abeloff’s Clinical Oncology. 6th ed. Philadelphia, PA: Elsevier; 2020:chap 69.
Arbour KC, Riely GJ. Systemic therapy for locally advanced and metastatic non-small cell lung cancer: A Review. JAMA. 2019;322(8):764-774. PMID: 31454018 www.ncbi.nlm.nih.gov/pubmed/31454018.
Colt HG, Murgu SD, Korst RJ, Slatore CG, Unger M, Quadrelli S. Follow-up and surveillance of the patient with lung cancer after curative-intent therapy: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 Suppl):e437S-454S. PMID: 23649451 www.ncbi.nlm.nih.gov/pubmed/23649451.
Ettinger DS, Wood DE, Aisner DL, et al. Non-small cell lung cancer, Version 5.2017, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2017;15(4):504-535. PMID: 28404761 www.ncbi.nlm.nih.gov/pubmed/28404761.
Greenhalgh J, Dwan K, Boland A, et al. First-line treatment of advanced epidermal growth factor receptor (EGFR) mutation positive non-squamous non-small cell lung cancer. Cochrane Database Syst Rev. 2016;(5):CD010383. PMID: 27223332 www.ncbi.nlm.nih.gov/pubmed/27223332.
Hanna N, Johnson D, Temin S, et al. Systemic therapy for stage IV non-small-cell lung cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol. 2017;35(30):3484-3515. PMID: 28806116 www.ncbi.nlm.nih.gov/pubmed/28806116.
Herbst RS, Morgensztern D, Boshoff C. The biology and management of non-small cell lung cancer. Nature. 2018;553(7689):446-454. PMID: 29364287 www.ncbi.nlm.nih.gov/pubmed/29364287.
Howington JA, Blum MG, Chang AC, Balekian AA, Murthy SC. Treatment of stage I and II non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 Suppl):e278S-e313S. PMID: 23649443 www.ncbi.nlm.nih.gov/pubmed/23649443.
Khuri FR. Lung cancer and other pulmonary neoplasms. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 26th ed. Philadelphia, PA: Elsevier; 2020:chap 182.
Marmarelis M, Thompson JC, Aggarwal C, et al. Emerging uses of circulating tumor DNA in advanced stage non-small cell lung cancer. Ann Transl Med. 2017;5(18):380. PMID: 29057240 www.ncbi.nlm.nih.gov/pubmed/29057240.
Mazzone PJ, Silvestri GA, Patel S, et al. Screening for Lung Cancer: CHEST Guideline and Expert Panel Report. Chest. 2018;153(4):954-985. PMID: 29374513 www.ncbi.nlm.nih.gov/pubmed/29374513.
Osmani L, Askin F, Gabrielson E, Li QK. Current WHO guidelines and the critical role of immunohistochemical markers in the subclassification of non-small cell lung carcinoma (NSCLC): Moving from targeted therapy to immunotherapy. Semin Cancer Biol. 2018;52(Pt 1):103-109. PMID: 29183778 www.ncbi.nlm.nih.gov/pubmed/29183778.
PDQ Adult Treatment Editorial Board. Non-small cell lung cancer treatment (PDQ®): Health Professional Version. PDQ Cancer Information Summaries [Internet]. Bethesda (MD): National Cancer Institute (US); 2002-.2019 Jun 13. PMID: 26389304 www.ncbi.nlm.nih.gov/pubmed/26389304.
Ramnath N, Dilling TJ, Harris LJ, et al. Treatment of stage III non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 Suppl):e314S-e340S. PMID: 23649445 www.ncbi.nlm.nih.gov/pubmed/23649445.
Rigotti NA. Balancing the benefits and harms of E-cigarettes: A National Academies of Science, Engineering, and Medicine Report. Ann Intern Med. 2018;168(9):666-667. PMID: 29435573 www.ncbi.nlm.nih.gov/pubmed/29435573.
Rivera MP, Mehta AC, Wahidi MM. Establishing the diagnosis of lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based Clinical practice guidelines. Chest. 2013;143(5 Suppl):e142S-e165S. PMID: 23649436 www.ncbi.nlm.nih.gov/pubmed/23649436.
Silvestri GA, Pastis NJ, Tanner NT, Jett JR. Clinical aspects of lung cancer. In: Broaddus VC, Mason RJ, Ernst JD, et al, eds. Murray and Nadel's Textbook of Respiratory Medicine. 6th ed. Philadelphia, PA: Elsevier Saunders; 2016:chap 53.
US Preventive Services Task Force, Krist AH, Davidson KW, Mangione CM, et al. Screening for lung cancer: US Preventive Services Task Force recommendation statement. JAMA. 2021;325(10):962-970. PMID: 33687470 pubmed.ncbi.nlm.nih.gov/33687470/.
Review Date: 12/13/2019
Reviewed By: Todd Gersten, MD, Hematology/Oncology, Florida Cancer Specialists & Research Institute, Wellington, FL. Review provided by VeriMed Healthcare Network. Also reviewed by David Zieve, MD, MHA, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. Editorial update 08/02/2021.
